
By Dr. Alison McAllister, ZRT Laboratory
This article tackles some frequent questions providers might have regarding the purpose of the testing and who the ideal patient is.
TESTING SPECIFICS
Why urine testing instead of saliva?
- Saliva testing is what ZRT was founded on, and we have tested over 1.8 million individuals at this point. We are celebrating 20 years of hormone testing this year! Hurray! We love saliva testing. But, what we don’t love is having you collect every other day for 15 samples. Urine testing has the benefit of a super easy collection – wake up and pee on the strip! If you forget that time, you do your second morning urine. Easy.
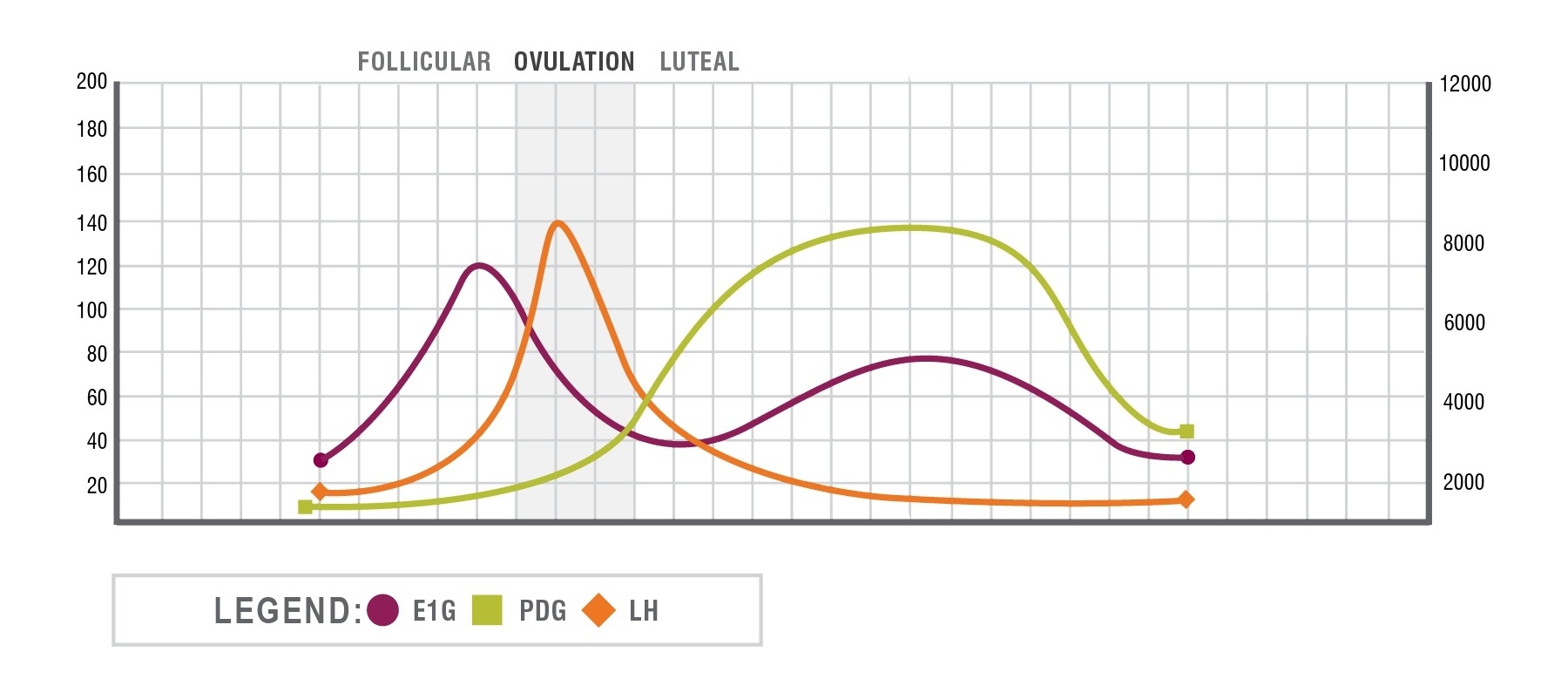
- Urine testing is also well established in the medical literature for the purpose of this test, which is determining ovulation, LH, estrogen, and progesterone levels. Saliva would also work, but we can’t test LH to help pin-point LH; Bloodspot works really well, but ouch, too many finger pokes. Since we are looking for patterns more than absolute levels, urine is the perfect, easy collection tool.
Blood on the strip – is this a problem?
- No! We are testing metabolites of estrogen and progesterone that are generated by the liver and rapidly eliminated in urine. Thus, the levels in any blood contamination will not skew the patterns.
Can I change the time my patient collects the samples?
- Absolutely! Our default is 15 strips provided in the kit. We encourage starting on day 7 and continuing on alternate days until the period appears. For many women that means that about 11 samples will be collected. If your patient has a 28-day cycle, that means you have an additional 4 strips that you could have collected when the patient’s symptoms are at their worst or when you would like to see more data points. ZRT will be plotting all information relative to the actual days of the cycle when the samples were collected.
Pooling samples? Other labs pool the samples but have the patient collect every day; do you do this?
- ZRT does not pool samples. It is not in the interest of patients to have averages of hormone levels over 2 or more days reported back to them. Pooling a sample that is low on day 10 with a sample that is high on day 12, for instance, would produce a “normal” result, yet the highs and low are what could be behind the patient’s symptoms – i.e., drops in estrogen that can trigger migraines. Assessing levels on the actual days gives the best information for the patient.
Miss a day?
- If a patient misses a morning, they can do it later that same day OR just collect the next day as well as the following day to get back on the same pattern. For example, if Sunday was missed, they would collect Monday to compensate, and then test on Tuesday as originally planned.
Card damaged?
- If a patient damages a card (e.g. drops in the toilet etc), just have them use another card to collect the second morning sample or collect the next day. Most women (with average cycle of 28 days) will only expect to use 11-12 cards, so there should be several extra urine cards for them.
PATIENT CONDITIONS
Who is the ideal patient?
- I think any woman would enjoy the information that they get from this test. It’s fun to see how much our hormones fluctuate, when ovulation happens, and what progesterone is doing in the luteal phase. So, given all of that, I think the woman who is having symptoms associated with menstrual hormone changes throughout the month, women dealing with infertility, irregular spotting or migraines are the women most likely to benefit from this information.
Ablations
- Yes, this test might be great for women who have had an ablation, are having symptoms, and have no idea where their cycles are. It would generally be able to help them determine at what stage of their cycles they are.
Amenorrhea/No Periods
- If you want to do Menstrual Cycle Mapping on amenorrheic patients, just have them choose a random day and collect every other day until all 15 cards are collected. If they have had an ablation or hysterectomy and have symptoms associated with their “period time,” then they can count that as the period and start collecting after that until all cards are filled.
- Saliva or blood spot testing is another way of testing these patients with a single collection.
Is this kit the same as ZRT's Fertility kit?
- This kit is not the same as ZRT's Fertility Profile which measures estradiol, progesterone, testosterone, DHEAS, FSH, diurnal cortisol, and thyroid hormones. It’s designed to help a patient evaluate for ovarian potential as well as screen for many conditions that inhibit fertility like hypothyroidism, PCOS, and low vitamin D. When used for fertility purposes, the Menstrual Cycle Mapping kit is designed to help a woman understand the fluctuations in her hormones during the month that may contribute to inadequate uterine lining, the lack of ovulation, or inadequate luteal progesterone levels. While the Cycle Mapping kit will show if a woman has ovulated, it doesn’t give the full range of hormones that the Fertility kit does.
- I think of these as synergistic to each other – both providing excellent, but not interchangeable information.
Can we test people on IUDs?
- As a lab, we can test anyone, but it might not clinically be helpful. Copper IUDs (not containing any hormones) will still show ovulation (or attempts to ovulate), estrogen, and progesterone levels. Progestin IUDs will show a flat progesterone level since the progestin won’t be seen by the assay, but it will still show estrogen fluctuations and potentially LH fluctuations. For many women who don’t cycle at all on their progestin IUD, we may not see any progesterone or even LH fluctuations. I’ll update this information if we can show what these women’s patterns tend to look like.
- For someone who has symptoms with the progestin IUD and has no periods, a single salivary or blood spot test should be adequate. If symptoms are fluctuating throughout the month with “good and bad” times then this test may be beneficial, but please understand the limitations of the test.
Oral contraceptives?
- I do not think this is a good test for women on hormonal contraceptives, even if they are symptomatic. If women are still getting heavy periods on contraceptives you might consider looking at tranexamic acid or use of NSAIDS as therapy. The ethinyl estradiol and progestins in the oral contraceptives will flatten the hormones in the test.
PCOS – Polycystic Ovarian Syndrome
- About 50% of women with PCOS will have a higher LH throughout the cycle. Women will tend to have anovulatory cycles and oligomenorrhea (few cycles). A single sample with saliva or blood spot is likely adequate, but women may enjoy checking to see if they are having any surges in progesterone or LH, or if they are ovulating, checking to see if they are having adequate progesterone levels in the luteal phase.
Progesterone supplementation: can I use this test to look at my progesterone dosages?
- We do not recommend using this test to look at supplementation. Topical supplementation isn’t going to be well represented in urine and oral supplementation is going to be overly represented due to progesterone metabolism in the liver. As a lab, we of course can test it, but this test might not answer the question that you need answered.
HORMONES QUESTIONS
Is it normal to have very strong, painful ovulation cramps?
- This is known as Mittelschmerz and is not uncommon. While many women have no symptoms of ovulation, some women will experience twinges of pain, cramping, spotting or any number of symptoms for minutes to hours around ovulation. This is thought to be due to the prostaglandin changes associated with ovulation.
TREATMENT QUESTIONS
Iron levels
- Iron supplementation is generally 325 mg/capsule or tablet in which 25 mg is elemental iron. While many anemic patients will have good replacement with as little as 1 capsule, many women with heavy periods will require much higher levels of iron supplementation. In my experience, if ferritin is very low and women have heavy bleeding they will often require or benefit from either IV iron infusions or injections and/or therapy to stop their heavy bleeding, even if that means using a progestin IUD or oral contraceptive to get on top of the blood loss and restore ferritin levels.
- Iron is required to optimize uterine cramping which is part of how the uterus stops the period, so women with low iron levels tend to bleed more because they can’t stop the period, thus leading to even more iron deficiency.
Curcumin for heavy bleeding?
- Sadly, there has been no research published on this topic. Curcumin is known to be a fibrinolytic, so if heavy bleeding is thought to be due to a blood disorder such as Von Willebrand’s, it should be used cautiously or avoided, just like NSAIDS which could contribute to increased bleeding. However, curcumin also manipulates prostaglandin production, like NSAIDS, and as such would be expected to help many women with heavy bleeding. Some studies suggest a 50% reduction of bleeding with NSAID usage. Many women have noted that curcumin helps decrease their heavy flows.
What about Tranexamic acid/Lysteda (oral)/Cyklokapron (injection) for heavy bleeding?
- Tranexamic acid is a relatively new medication for bleeding or I should say that it’s still relatively newish in using it for heavy bleeding in most practices. Tranexamic acid has been used by women with Von Willebrand’s to control bleeding disorders for many years. It is a non-hormonal treatment for heavy periods and is a synthetic lysine amino acid derivative. It reduces bleeding by 40% and was tested in women with a variety of causes of heavy periods including fibroids. The medication is only used for 1-5 days and only at the time of bleeding. Tranexamic acid works by slowing the action of fibrinolysis which can contribute to heavy periods. Sadly, it’s not suggested for women on hormonal contraceptives or who have a history of blood clots, as the therapy will increase clotting risk. Studies have shown that it can work as well as hormonal contraceptives for heavy bleeding at all age groups, so I think it’s a nice option to have especially for people intolerant to contraceptives. It is prescribed as 2 tabs (650 mg) TID for 1-5 days. Cash price is about $150/30 tablets. As a fun fact, this product is available over the counter in Britain and Japan for about $14 US/18 tablets. Totally try it for your patients!
I’m super excited to share with you examples of cycles as we review more and more of these. Don’t hesitate to contact us if a question hasn’t been answered. I hope you get lots of great information from this test.